
This publication has been issued by Denge Laboratories to indicate the issues that both the patient and the laboratory should pay attention to. While creating the content, the 2010 version of the Semen Analysis book of the WHO (World Health Organization), which is a reference for all infertility studies in the world, was taken as a basis for semen analysis principles.
Many factors, from sample collection to testing in the laboratory, affect the results and the treatment determined according to these results especially in the treatment of male infertility. In addition to the doctor administering the treatment and the laboratory performing the analysis, it is very important for the patient to be conscious in order to obtain accurate results. Being conscious of the person giving the sample eliminates the error factors before the analysis and provides orientation to the treatment with the most accurate result.
Why is Semen Analysis Performed?
There are two main reasons for semen analysis.
Measurement of the total number of spermatozoa: This parameter shows how much spermatozoa can be produced in the testicles and whether the channels through which the sperms will travel after they leave the testicles are blocked.
Features of spermatozoa (vitality, motility, morphology) and composition of seminal fluid
It is necessary to be sensitive to preanalytical and analytical factors in semen analysis. Deciding which path to follow for infertility treatment depends on the most accurate conclusion of sperm analysis by the laboratory.
Issues and Importance to Consider While Giving Sperm Sample
Preanalytical Factors
Giving the sperm sample in a different environment -in a container in the laboratory- manifests itself with different effects from normal sexual intercourse. Sperm conditions in the natural environment and in the laboratory are significantly different. For the most accurate results, this difference should be minimized.
The following factors affect semen analysis:
- Having the entire sample in the container: During ejaculation, the first fraction is the prostate fluid, which is rich in sperm. The next portion contains the seminal sac fluid. Therefore, having the first fraction in the container positively affects the result for detecting the rich sperm fraction.
- Previous duration of sexual activity: If there is no complete ejaculation in the previous ejaculation, some spermatozoa from the previous ejaculation remain in the epididymis. This may not make a significant difference in the number of old and young spermatozoa in the entire ejaculate, as long as it does not exceed the standard time (2 to 7 days) after ejaculation in general, but this information must be shared with the laboratory and included in the report.
- Things to consider when giving sample: If semen is to be used for microbiological analysis, the person should wash their hands and penis using soap and rinse the soapsuds thoroughly while giving sample. Not rinsing the soapsuds well and mix of them with the sample will kill the bacteria that will be produced and cause false negative results. Care should be taken to ensure that the container to be used is sterile. Analysis time should never exceed 3 hours.
- If the semen sampling will take place at home: Sperm sampling time and whether the entire ejaculate is in the container should be recorded, and the laboratory should be informed. The sample should be delivered to the laboratory within 1 hour at the latest. The sample should be kept at a temperature of 20 to 37 degrees Celsius during this time (holding under the armpit is usually appropriate for these conditions). If the sample will be in a condom, the condom must not contain any toxic content for sperm. Especially latex condoms should not be used.
Issues and Importance To Consider While Analyzing Sperm Sample
(Analytical Factors)
After the semen sample is taken, the following factors should be meticulously fulfilled to prevent analysis errors:
- Analysis must be started within 30 minutes
- Care should be taken to keep the lid of the sample container closed (due to the risk of dehydration)
- The decision should be made by analyzing multiple semen samples: Two or three samples should be analyzed to obtain baseline data. However, these samples must be given at the same sexual abstinence period for accurate comparison.
- Heat factor: The sample should be kept at a constant temperature of 20 to 37 degrees Celsius after ejaculation to protect it from large-scale temperature changes that may adversely affect the spermatozoa. While the sample is liquefied, it should be kept in an oven at 37 degrees Celsius. If this is not fulfilled, all factors in the laboratory analysis (mobility, viscosity, pH, liquefaction time, etc.) may be affected.
All information that can be obtained from the person must be reported in the laboratory result form:
- Sexual abstinence period
- Whether ejaculation is complete
- Whether all the ejaculate is in the container
- If the sample is brought from home, the time and temperature conditions since the sample was taken
- If the sample is brought from home, the characteristics of the sample container and how the container is supplied
- If the sample is in a condom, checking the packaging information of the condom about whether the condom is toxic to sperm.
- Confirmation of that the soapsuds were thoroughly rinsed at the time of sampling.
Semen Formation Physiology For The Enthusiasts
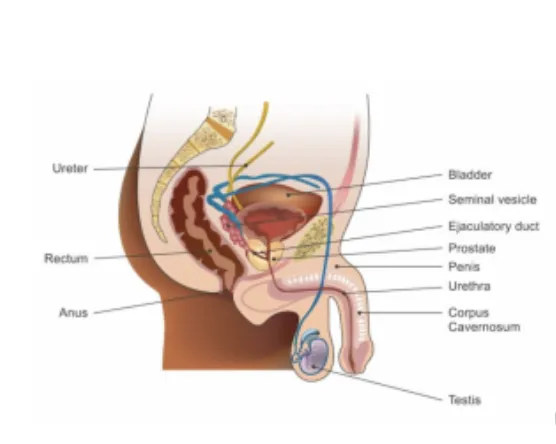
Sperm are produced by the testicles in the male body. The testicles are oval-shaped organs, each weighs 10 to 15 g, located just behind the penis, just in front of the anus. The testicles should be in a slightly cooler environment than body temperature in order to produce the most accurate sperm. Therefore, a flabby piece of skin called the scrotum around the testicles acts as a heat regulator that protects the testicles. The muscles in the scrotum relax and tighten, adjusting the proximity and distance of the testicles to the body, ensuring that they are not affected by body temperature.
The testicles produce 200,000 sperm per minute. However, from the age of 30, this number slowly decreases.
In addition to sperm, the testicles produce androgen hormones. Androgens are hormones that regulate sexual functions and govern the development and function of male anatomical organs. In a healthy man, an average of 6 milligrams of testosterone is secreted from the testicles per day.
Inside each testicle, there are are tubules containing the hormone testosterone, which is synthesized by Leydig cells, and Sertoli cells, which produce sperm. Sertoli cells are in the seminiferous tubules, which contain 23 chromosomes and produce sperm with the Y chromosome. These tubules also contain multiple blood and lymphatic vessels and nerve filaments. These tubules are tightly spiraled inside the testicles. Each testicle contains about 900 tubules. Their length is about 50 cm, and a seminiferous tubule, which is totally 800 meter-long in open state, is located in normal testicles. A fibrous tissue called cunica covers the tubules. This tissue contains 3 layers:
- Tunica vasculosa containing blood vessels and connective tissue
- The tunica albuginea, which surround the testicles and attaches the epididymis (the densely entwined appendage organ just behind the testicles that carries the sperm produced in the testicles to the penis) to the surrounding fibers
- Tunica vaginalis, which prevents friction between testicles and scrotum
Spermatogenesis (Formation Of Sperm)
Spermatogenesis is the formation of sperm in the seminiferous tubes of the testicles through meiosis. A sperm cell consists of genetic material with 2n chromosomes from the male reproductive system. Cells containing this material are called spermatogonia. These cells first proliferate in the same genetic structure through mitosis and are prepared for meiosis (division in a different genetic structure) after developing. These cells are called primary spermatocytes. At the end of meiosis, two cells with haploid (1n) chromosomes are formed from cells with 2n chromosomes. These cells are called secondary spermatids. At the end of the second meiosis, cells with 1n chromosomes are formed from the secondary spermatids. After this stage, sperms are formed through differentiation.
While the sperm cells are immature at first, Sertoli cells continue to supply them with blood products and the mature cells are transported up to the central canal of the seminiferous tubules. After reaching the epididymis, spermatozoa wait for maturation for about 20 days. These are carried to the penis via the ductus deferens for ejaculation.
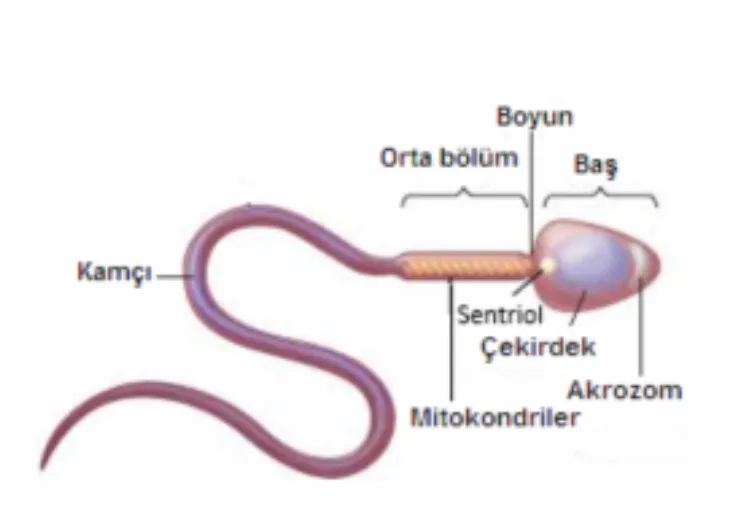
Maturation is essential to fertilize the egg, and after the development of the genetic information contained (when meiotic, mitotic divisions are complete) a condensed and oval head is formed. A cap on this head, called the acrosome, allows it to enter the egg’s shell.
There is a tail at the back of the head. This tail is produced from the cytoplasm of the sperm in the second developmental stage. Mitochondria are located in the middle of the sperm. The ATP energy generated by the mitochondria is used by the microtubules that form the structure of the tail, and the energy of movement emerges.
The tail allows the sperm to move towards the egg to carry out fertilization.
What Is In The Semen Sample?
The semen sample is a suspension containing spermatozoa and seminal plasma. The seminal plasma ensures that the sperm cells are kept alive. The semen volume of a normal man is 2-5 ml on average and there are 200 to 300 million spermatozoa in each ejaculation.
The liquid part of the semen out of the sperm forms its first component with a liquid containing potassium, sodium and glycerophosphoryl choline, which is the energy source for the sperm, in the epididymis. Sperm that mature in the epididymis pass through the ductus deferens or vas deferens to another waiting area called the ampulla. Here, ergothioneine (yellow, oxygen-destroying substance in chemicals) and fructose (sugar that enriches sperm’s energy) are added to it.
Prostate fluid and fluid in the seminal tubes also participate in ejaculation. Thus, the sperm concentration is diluted and becomes fluid. Prostate and seminal fluids contain fructose, amino acids, citric acid, phosphorus, potassium and hormones called prostaglandins. Of the total fluid, seminal fluid constitutes 60% while prostate fluid constitutes 30%. Prostate fluid contains citric acid, acid phosphatase, calcium, sodium, zinc, potassium, protein chain breaking enzymes and fibrolysin (enzyme that reduces blood and tissue strands).
There is magnesium, sufficient oxygen in the plasma, suitable temperature and a slightly alkaline pH (between 7-7.5) to enable the sperm itself to move.
Sulfate crystals in semen prevent sperm from expanding.
Fructose is the main nutrient that provides energy to the sperm cell. Semen also contains a protein called mucus from the bulbourethral and urethral glands that is thick, clear and lubricating.
Information for the laboratory: Semen Analysis
Liquefaction
Normal limits: 15 to 60 minutes
Semen is in the typical semi-solid coagulated form immediately after ejaculation. It begins to liquefy within a few minutes at room temperature. The entire sample should be liquefied within 15 minutes at room temperature. This can rarely take up to 60 minutes. If there is no liquefaction, it should be reported. As long as the semen is liquefied, the amount of motile sperm will increase. Therefore, macroscopically, liquefaction should be properly observed and analysis should be started after that. Samples prepared at home will probably have been liquefied until they arrive at the laboratory. Even if there are immobile spermatozoa at the first observation, a little more liquefaction can be expected. During this time, the process can be assisted by gently mixing the sample at 37 degrees. For some samples, the process can be assisted by adding an equal amount of physiological medium or bromelin enzyme. Details of these processes are specified in WHO Standards 2010.
Viscosity
Normal limits: Less than 2 cm
Normal semen is aspirated into a plastic pipette with a diameter of approximately 1.5 mm immediately after liquefaction and an viscosity is estimated by observing the filamentous appearance of the drop formed by gravity. If the viscosity is abnormal, filaments longer than 2 cm are formed.
Appearance
Normal appearance: Gray-opalescent
A normal semen sample appears gray-opalescent (semi-opaque). It may have a less opaque appearance if the sperm concentration is too low. If erythrocytes are present (hemospermia), it appears red-brown and may appear yellowish if the person is icteric or is taking certain medications and vitamins.
Volume
Normal limits: >1.5 ml
Its volume is made up of fluids from the seminal sacs and prostate, and some from the bulbourethral glands and epididymis. Accurate evaluation of the volume is very important because the number of spermatozoa is reported by comparing the total volume of semen and the number of non-sperm cells. The healthiest method for volume measurement is to weigh the container together with the semen sample and then to weigh it as empty. When the weight of the container is subtracted, the volume can be calculated according to the gr/ml ratio, using the formula density = total weight / total volume, assuming the semen density is 1 gr/ml. The volume can also be read by transferring the semen sample directly from the graduated glass to the measuring cylinder, but a decrease of 0.3-0.9 ml should be taken into account as the sample volume remaining at the rim of the container during transfer.
If the volume is low, an obstruction of the ejaculatory duct or underdevelopment of the seminal sac can be considered (congenital absence of bilateral vas deferens). Or, there may be loss of part of the sample during ejaculation or androgen deficiency.
Conversely, high semen volume may reflect the excretion of excess fluid as a result of inflammation of peripheral organs.
pH
Normal value: >7.2
Semen pH indicates the balance between alkaline seminal sac secretion and acidic prostate secretion. The pH value should be measured after 30 minutes of liquefaction. Since the CO2 production of spermatozoa is constantly increasing, the measurement should be completed within 1 hour after sampling. The measurement is made using pH paper.
Microscopic Analysis
The initial microscopic analysis of the sample uses x100 magnification (combination of x10 objective and x10 magnification eyepiece). In this way, mucus, filament formation, sperm aggregation and agglutination, presence of non-spermatozoal (epithelia, leukocytes, immature germ cells, isolated heads and tails) can be detected.
x200 and x400 magnifications are used in the second stage analysis (combination of x10 eyepieces with x20 or x40 objective). Sperm motility is evaluated at this stage. Different dilutions can be tried while counting sperm. It is important to mix the sample by gently pipetting and releasing (10 times with a plastic pipette of 1.5 mm). If it is not done, erroneous assessments of sperm (motility), vitality, concentration and morphology can be made.
After mixing, approximately 10 microliters of semen sample is placed on a clean slide so as not to allow the spermatozoa to settle in suspension. Thus, a preparation with a constant depth of approximately 20 microliters is created with a 22×22 coverslip. The weight of the coverslip allows the sample to spread on the slide. A chamber depth of less than 20 microliters limits the rotational movements of the spermatozoa. In the case of a deeper chamber, counting will be difficult as the spermatozoa will move freely in and out of the focal area. The sample is nonhomogeneous if the number of spermatozoa varies markedly in each visual field. Another sample should be prepared.
The ejaculate contains non-spermatozoal cells, some of which may be clinically significant. Leukocytes and immature germ cells are called “round cells”.
Sperm Motility
Sperm motility is the most common category as progressive motile (30-50%), non-progressive motile (5-15%) and immotile (35-65%).
The rate of progressive motility of sperm is closely related to pregnancy. Sperm motility of the semen should be evaluated within one hour at the latest after liquefaction. In this way, the negative effects of pH, dehydration and temperature changes on sperm motility are eliminated.
Motility should be checked at 37 degrees, and it is important to keep the semen in an oven at 37 degrees for the specified time, and to ensure that the slides and coverslips are also at 37 degrees. First, those that with progressive motility, then those with motile in place and those that are non-motile are evaluated. The motility of each spermatozoa is graded as follows:
- Progressive motility / PR: It is the number of actively motile spermatozoa in a linear or wide circle, regardless of speed.
- Non-progressive motility / NP): All other types of motility where there is no forward movement. For example, swimming in small circles, movement in the head or just the flagellum movement of the tail can be observed.
- Immotility / IM): Complete stagnation. Note: In previous versions of the World Health Organization standards, it was recommended to classify spermatozoa with progressive motility according to fast or slow motility. Accordingly, it was suggested that spermatozoa, which can move 25 micrometers per second, should be named Grade A. However, it is not possible for a technician to measure progressive motility that well. Instead, at least 200 spermatozoa are evaluated at least in 5 areas. The mean percentage is calculated for the most common degree of motility (Pr, NP or IM). If the difference between the percentages is acceptable (otherwise the sampling is repeated), the mean percentages of the degree of motility are reported. The average of intact spermatozoa with only one head and one tail is selected. The mean percentage in each motility category may be rounded to the nearest integer. To evaluate sperm motility, it would be correct to use a graduated eyepiece and choose an area of at least 5 mm from the edge of the coverslip to the inside.
- The number of spermatozoa with progressive motility in the ejaculate: It is obtained as a percentage of the total number of sperm in the ejaculate multiplied by the number of sperm with progressive motility.
Vitality
Normal value: The reference lower limit of vitality is more than 58% intact cells.
Sperm vitality is the degree of viability of sperms determined by the integrity of the cell membrane. Vitality analysis is important if sperms with progressive motility is less than 40%. This test can also check the accuracy of motility. Cells with intact membranes are identified and evaluated by the eosin dye retention or hypoosmotic swelling test.
If the cells retain dye, it is understood that those cells are dead. The hypoosmotic swelling test has the principle that only living cells with intact membranes will swell in hypotonic fluids. The presence of viable but immotile cells may indicate structural problems in the sperm tail. Immotile and non-viable cells (necrozoospermia) may be indicative of epididymal pathology. In the eosin-nigrosine staining technique, color differences between the background and the sperm heads suggest that the sperm are dead or alive. Red-headed–D1 or pink-headed–D2 spermatozoa are considered dead and white-L or slightly pink-headed spermatozoa are considered viable membranes. The presence of nigrosine dye provides a dark background and is necessary to see even lightly stained sperm. If the dye is limited only to the neck area and the rest of the head is not stained, it is called leaky neck membrane and the cell is not considered dead.
The number is obtained by multiplying the total number of spermatozoa in the ejaculate with the percentage of cells with intact membranes. The hypoosmotic swelling test (HOS) is an alternative test for membrane integrity. Sperm with intact membranes swell in 5 minutes in a hypoosmotic environment. Swollen spermatozoa are noticeable by changes in cell shape, such as the tail becoming spiraled.
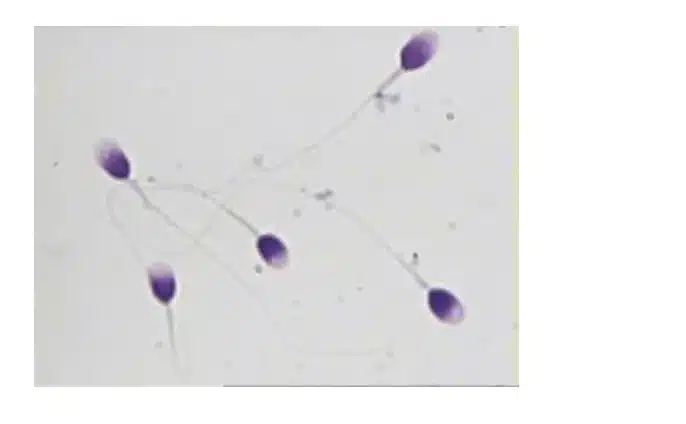
Sperm Morphology
Normal limits: Although the percentage of sperm with normal morphology is considered to be 10-14%, the lower limit is accepted as 4%.
Determining the percentage of normal or abnormal forms of sperm morphology is important for deciding the fertility program. The percentage of normal values in both fertile and infertile men ranges from 0 to 30% and exceeds 25% in a small number of samples. Reference limits of 3-5% have been established in intrauterine insemination or in-vivo fertility studies.
Under detailed field microscopy, the acrosomal region of the head is stained light blue and the post-acrosomal dark blue. The middle segment may retain some red dye. The tail may retain a blue-reddish color. Usually the back of the head may retain a resident cytoplasmic remnant or a reddish-orange color (with Papanicolaou, Shorr stains).
The sperm consists of a head, neck, middle piece, main piece and end piece. Since the last piece is difficult to see under the light microscope, it can be thought of as consisting of a head, neck and tail. When evaluating whether sperm are morphologically normal or not,
- The head and tail should be normal. Shapes in range are considered abnormal.
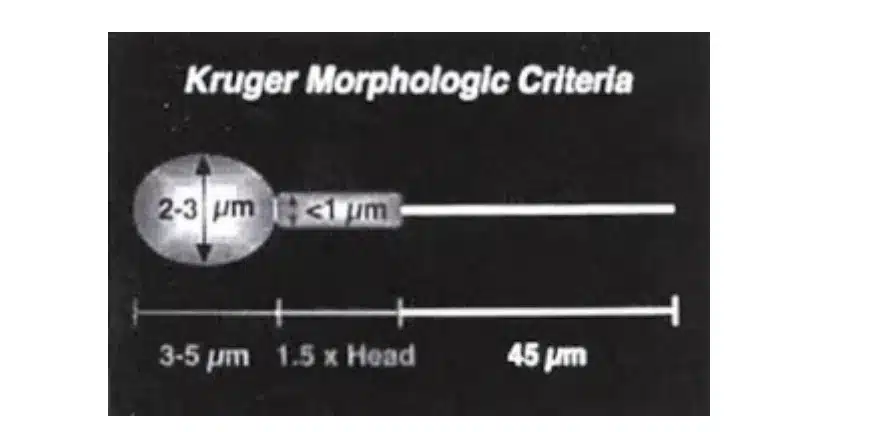
- The head should be smooth, has smooth contour and generally oval in shape.
- The acrosome region should contain no more than two small vacuoles and should not cover more than 20% of the sperm head.
- The post-acrosomal region should not contain any vacuole.
- The middle piece should be thin, has smooth contour and approximately the length of the sperm head.
- The main piece should be the same width throughout its length, thinner than the middle piece and approximately 45 micrometers long (about 10 times the head length).
- Unless there is a definite angle indicating that the tail is broken, it can curl backwards on itself in a loop.
Defective spermatogenesis and some epididymal pathologies are often associated with increased percentages of abnormally shaped sperm. Abnormal sperm usually have a low fertilization potential, depending on the types of anomalies, and their DNA may also be abnormal. Morphological defects may be indicative of increased DNA fragmentation process, structural chromosome abnormalities and increased aneuploidy. Therefore, the shape of the head is particularly emphasized, although the sperm tail is considered.
In microscopic morphology analysis of semen, polymorphonuclear leukocytes can sometimes be confused with spermatids. However, they may appear bluish when compared to the pinkish color of the spermatids. The experience of the analyzer technician is important here (another way to define the leukocyte population in semen is to determine peroxidase activity by staining with ortho-toludine and is reliable only in separating polymorphonuclear leukocytes from spermatids). Peroxidase in the ejaculate may reflect the severity of the inflammatory condition.
The presence of too many leukocytes in the ejaculate (leukocytospermia, pyospermia) indicates infection and poor sperm quality. Leukocytes can impair sperm motility and DNA integrity through oxidative attack.
Antibodies In Semen
Evaluation of normal antibodies: Detection of motile sperms by 50% is accepted as a general trend. If 50% or more motile sperm are bound to antibodies, in-vivo fertilization is impaired.
There are two immunoglobulin antibodies in semen, IgA and IgG. These are called Anti-Sperm Antibodies (ASA). These tests are called Direct Tests (Mixed Antiglobulin reaction: MAR test). Another test is the Immunobead Test (IB). The results of the IB test correlate well with the immobilization test, which detects antibodies in the serum. Although the experimental protocols of the IB and MAR tests vary, the sperm/bead preparation is analyzed by means of a microscope. The beads adhere to motile and immotile sperm with antibodies bound to the surface and the percentage of motile sperm bound to the beads is recorded.
Germ cells
Both round spermatids and spermatocytes rarely contain spermatogonia. Although they can be detected in stained semen swabs, when cells degenerate, they can be difficult to distinguish from inflammatory cells. They can be recognized and separated by staining with Papanicolaou dye.
Computer-Assisted Sperm Analysis (CASA) and Manual Analysis Methods
ESHRE (European Society of Human Reproductive Medicine) reported in 1998 that sperm measurement with the device was not appropriate due to the difficulties of separating sperm from other cells. However, it reported in 2003 that this method could also be used through careful sample preparation, the use of fluorescent dyes, and very careful calibration. Semen is a biologically active sample. For motility evaluation with devices, kinematic analysis methods should be applied. For evaluation of sperm morphology by means of devices (CASMA), it is essential, as always, to perform preparations and quality control. In particular, reproducibility, degree of accuracy, focusing, lighting, methodological changes in sample preparation and staining are important for the accuracy of the results.












